Hola amigos de HIVE, les traigo mi iniciativa y uno de mis sueños desde estudiante que espero ir puliendo y mejorando con ustedes con el paso del tiempo, y eso es crear animaciones médicas que expliquen procesos de mi carrera tanto teorícos cientificos para los que esten en la carrera, como para para pacientes. Quizá tarde un poco en crear contenido ya que es un poco díficil saber como expresar ciertas cosas y también a como organizarme para publicar pero al menos este año como médico interno trataré de hacerlo lo más que pueda.
Mi trabajo es realizado en la aplicación illustrator cs6 de mi autoría, serán presentados diversos personajes ya sean de creación propia como de animes, quienes serán nuestros protagonistas. Sin más que agregar los invito a apoyarme en mi instagram también donde de igual manera publicaré el contenido y muchas cosas más. Si siento mucho apoyo me motivarían a seguir publicando más continuamente.
Hello friends of HIVE, I bring you my initiative and one of my dreams since I was a student that I hope to polish and improve with you over time, and that is to create medical animations that explain processes of my career, both theoretical and scientific, for those who are in the race, as for for patients. It may take a while to create content since it is a bit difficult to know how to express certain things and also how to organize myself to publish but at least this year as an internal doctor I will try to do it as much as I can.
My work is done in the illustrator cs6 application of my authorship, various characters will be presented, whether they are of my own creation or anime, who will be our protagonists. Without further ado, I invite you to support me on my instagram, where I will also publish the content and many more things. If I feel a lot of support, they would motivate me to continue publishing more continuously.
Imagen realizada en illustrator cs6 de mi autoria.
Image made in illustrator cs6 of my authorship.
Se trata de escolar masculino de 11 años de edad quien acude a la emergencia del hospital militar (por su afiliación a dicha institución y el servicio médico quirúrgico gratuito que ofrece la misma) referido por un cirujano pediatría por un diagnostico presuntivo de abdomen agudo quirúrgico de tipo apendicitis.
Hablando un poco sobre apendicitis aguda se define como la inflamación del apéndice, ya que toda palabra medica con sufijo “itis” significa inflamación. Esta es la emergencia quirúrgica más frecuente en niños con una incidencia máxima en pacientes escolares de entre 9 a 12 años.
Se puede producir de diversos modos en donde la obstrucción del órgano y la causa vírica son las más probables, y se han encontrado causas obstructivas de hasta pequeños fragmentos de heces (fecalitos o coprolitos) que obstruyen la luz del órgano, así como también de semillas, huesos, vegetales, y formas parasitarias como Enterobius vermicularis, Entamoeba histolytica, Schistosoma mansoni, Strogyloides stercolaris, como causa más frecuente entre las formas de presentación víricas se debe por la hiperplasia linfoide de la zona que obstruye la luz y la zona circundante al órgano. Estas son las causas más frecuentes en edades pediátricas a diferencia de la edad adulta cuya causa más frecuente aparte de las obstructivas, con una disminución de la frecuencia por hiperplasia linfoide tenemos las de origen tumoral, a los pacientes que se han sometido a intervenciones quirúrgicas la presencia de bridas o adherencias pueden ser una causa.
Los síntomas de esta emergencia quirúrgica son un dolor abdominal que generalmente inicia a nivel del epigastrio (a nivel del estómago) y luego se irradia a las pocas horas a fosa iliaca derecha (región inferior derecha abdominal) y el dolor suele estar acompañado de inapetencia, nauseas, vómitos y fiebre.
Los signos más importantes empiezan desde la expresión del paciente, que suele tener una fascie de dolor, asimismo una marcha antalgica o dolorosa, los pacientes suelen llegar al consultorio encorvados, cojeando o negándose a deambular.
Cuando se examina el abdomen y se escuchan los ruidos propios del abdomen se escucha que están en total silencio, no hay presencia de movimientos en las asas intestinales por lo que los ruidos hidroaereos abdominales están ausentes y a nivel de la fosa iliaca derecha suele haber hipertermia (aumento en la temperatura en el área), al palpar suele haber una contractura involuntaria por reflejo. El dolor se enfoca en la fosa iliaca derecha en un punto doloroso llamado Mcburney que cuando se toca y duele se dice que esta positivo, y cuando duele al descomprimir se debe a la irritación del peritoneo y la posibilidad de peritonitis aumenta (signo de Blumberg: dolor a la descompresión en el punto de Mcburney), el signo del psoas esta positivo con dolor a la flexión del mismo por sobre el abdomen, signo del obturador; dolor a rotación interna de la rodilla.
En el examen paraclínico solemos encontrar una leucocitosis con neutrofilia en la ecografía abdominal puede hallarse engrosamiento de la pared apendicular y distensión de la luz del órgano (diámetro mayor de 6 m, plastrón o absceso local, presencia de líquido periapendicular, apendicolito, y asas intestinales inmóviles.
Radiografía simple del abdomen de pie: básicamente en el diagnóstico de apendicitis aguda. Puede ser útil en el diagnóstico cuando no se tiene otra ayuda diagnostica y se tiene duda. El hallazgo de fecalitos o apendicolitos calcificados en un niño con dolor agudo en cuadrante inferior derecho es muy sugestivo de apendicitis aguda, la presencia de niveles hidroaéreos en cuadrante inferior derecho (asas “centinelas”), escoliosis antiálgica derecha, borramiento de la sombra del músculo psoas o de la línea preperitoneal grasa del lado derecho.
El diagnóstico de la apendicitis es clínico y el tratamiento es quirúrgico, con apendicetomía. (Extracción del apéndice)
This is an 11-year-old male schoolboy who goes to the emergency room of the military hospital (because of his affiliation with said institution and the free surgical medical service that it offers) referred by a pediatric surgeon for a presumptive diagnosis of acute surgical abdomen of appendicitis type.
Speaking a little about acute appendicitis, it is defined as the inflammation of the appendix, since every medical word with the suffix "itis" means inflammation. This is the most frequent surgical emergency in children with a maximum incidence in school patients between 9 and 12 years of age.
It can be produced in various ways where the obstruction of the organ and the viral cause are the most likely, and obstructive causes have been found from even small fragments of feces (fecalites or coprolites) that obstruct the lumen of the organ, as well as from seeds , bones, vegetables, and parasitic forms such as Enterobius vermicularis, Entamoeba histolytica, Schistosoma mansoni, Strogyloides stercolaris, as the most frequent cause among the forms of viral presentation is due to lymphoid hyperplasia of the area that obstructs the light and the area surrounding the organ . These are the most frequent causes in pediatric ages, unlike in adults whose most frequent cause apart from obstructive ones, with a decrease in frequency due to lymphoid hyperplasia, we have those of tumor origin, in patients who have undergone surgical interventions the presence of flanges or adhesions can be a cause.
The symptoms of this surgical emergency are abdominal pain that generally begins at the level of the epigastrium (at the level of the stomach) and then radiates within a few hours to the right iliac fossa (lower right abdominal region) and the pain is usually accompanied by loss of appetite, nausea, vomiting and fever.
The most important signs start from the patient's expression, which usually has a fascia of pain, also an antalgic or painful gait, patients usually arrive at the office hunched over, limping or refusing to walk.
When the abdomen is examined and the sounds of the abdomen are heard, they are heard to be totally silent, there is no presence of movement in the intestinal loops, so the abdominal hydro-aerial sounds are absent and at the level of the right iliac fossa there is usually hyperthermia ( increase in temperature in the area), when palpating there is usually an involuntary reflex contracture. The pain is focused on the right iliac fossa in a sore point called Mcburney that when touched and hurts is said to be positive, and when it hurts when decompressing it is due to irritation of the peritoneum and the possibility of peritonitis increases (Blumberg's sign: pain on decompression at Mcburney's point), the psoas sign is positive with pain on flexion over the abdomen, obturator sign; internal rotation pain of the knee
In the paraclinical examination, we usually find leukocytosis with neutrophilia. In abdominal ultrasound, thickening of the appendicular wall and distension of the organ lumen can be found (diameter greater than 6 m, plastron or local abscess, presence of periappendiceal fluid, appendicolith, and intestinal loops). motionless
Plain X-ray of the abdomen standing: basically in the diagnosis of acute appendicitis. It can be useful in the diagnosis when there is no other diagnostic aid and there is doubt. The finding of fecaliths or calcified appendicoliths in a child with acute pain in the right lower quadrant is highly suggestive of acute appendicitis, the presence of air-fluid levels in the right lower quadrant ("sentinel" loops), right antalgic scoliosis, effacement of the muscle shadow psoas or the preperitoneal fat line on the right side.
Diagnosis of appendicitis is clinical and treatment is surgical, with appendectomy. (Appendix removal)

Imagen realizada en illustrator cs6 de mi autoria.
Image made in illustrator cs6 of my authorship.
This patient has a current disease of 4 days of evolution when the disease began on 03/04/22, after having a copious meal (grains) he presents abdominal distention and pain at the level of the epigastrium (at the level of the stomach) insidious, colic type, of moderate intensity, concomitant nausea. On 03/11/21 the pain is exacerbated and radiates to the right iliac fossa, concomitant loss of appetite, and absence of evacuation for 02 days, so he goes to a private health practitioner who evaluates and later goes to our center.

Imagen realizada en illustrator cs6 de mi autoria.
Image made in illustrator cs6 of my authorship.
El paciente tenía varios síntomas que nos hacían pesar en una causa no quirúrgica, un paciente que refería mucha ingesta de grasas, comidas abundantes, con poca cantidad de fibras y poca ingesta de agua, sedentario, que inicia el dolor justo después de ingerir una comida abundante, 4 días de enfermedad actual si la causa adyacente fuese una apendicitis el paciente ya estaría en un estado avanzado de la presentación y no había presentado vómitos, fiebre, el paciente se encontraba en buen estado general.
The patient had several symptoms that made us weigh in a non-surgical cause, a patient who referred a lot of fat intake, abundant meals, with little fiber and little water intake, sedentary, who started the pain just after eating a meal abundant, 4 days of current illness if the adjacent cause was appendicitis, the patient would already be in an advanced stage of presentation and had not presented vomiting, fever, the patient was in good general condition.
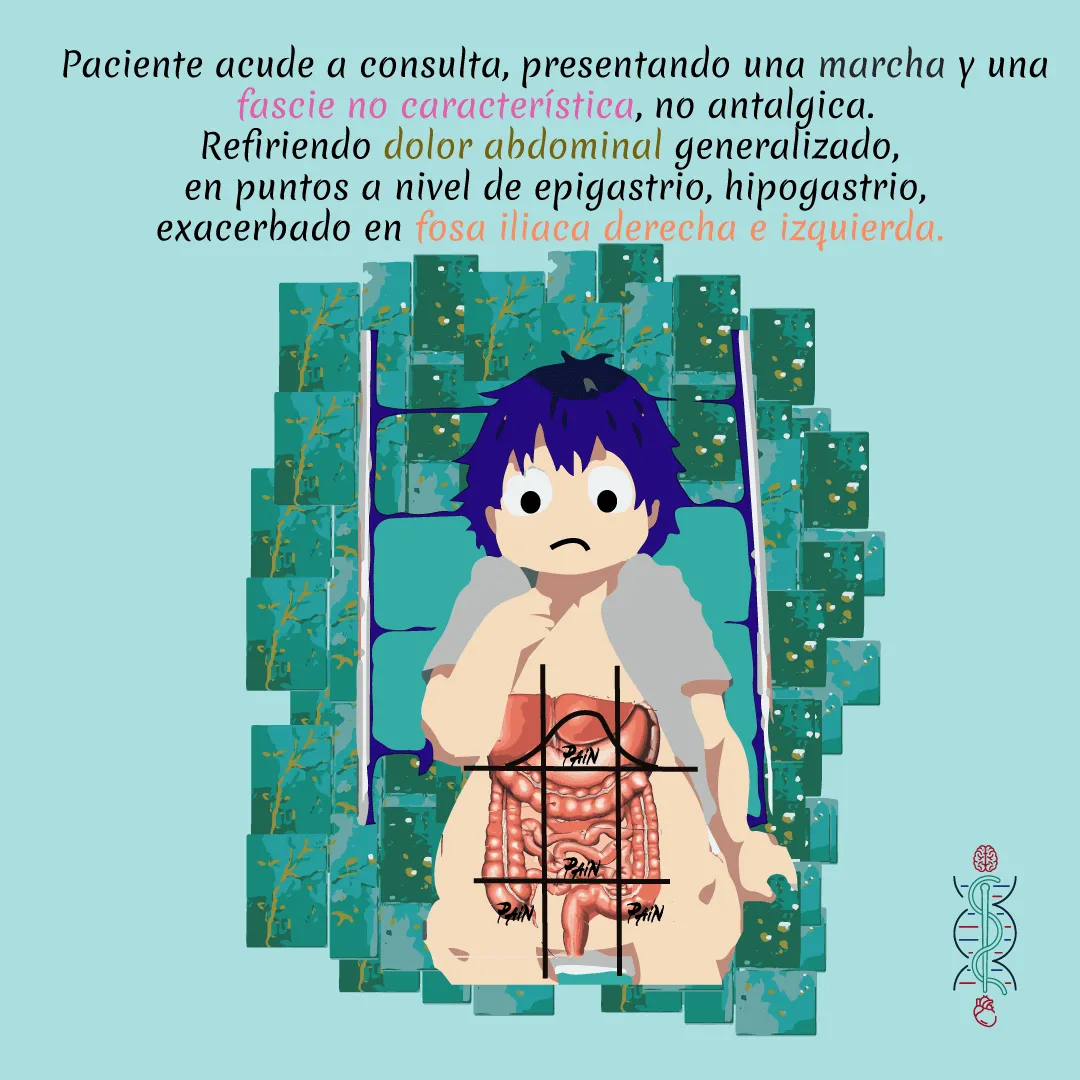
Imagen realizada en illustrator cs6 de mi autoria.
Image made in illustrator cs6 of my authorship.
Aun cuando el paciente presentaba el dolor de predominio en fosa iliaca derecha tenía otros puntos dolorosos de importancia a nivel de epigastrio, umbilical y fosa iliaca izquierda. Y el dolor no era de fuerte intensidad ya que se le ofreció quedarse en la camilla en espera de que sus padres regresaran y él decidió ir caminando sin ningún problema a buscar a sus padres, solo había dolor a la palpación.
Even though the patient presented pain predominantly in the right iliac fossa, he had other important painful points in the epigastrium, umbilical and left iliac fossa. And the pain was not of great intensity since he was offered to stay on the stretcher waiting for his parents to return and he decided to walk without any problem to look for his parents, there was only pain on palpation.

Imagen realizada en illustrator cs6 de mi autoria.
Image made in illustrator cs6 of my authorship.
Al examen físico el abdomen se encontraba globoso a expensas de panículo adiposo, distendido, con ruidos hidroaereos presentes, timpánico, blando y deprimible, doloroso a la palpación en fosa iliaca derecha, izquierda, región umbilical y epigástrica.
On physical examination, the abdomen was globular at the expense of the adipose panniculus, distended, with hydro-air noises present, tympanic, soft and depressible, painful on palpation in the right and left iliac fossa, umbilical and epigastric region.

Imagen tomada con cámara de celular poco M3 pro 5 G
Al examen físico el abdomen se encontraba globoso a expensas de panículo adiposo, distendido, con ruidos hidroaereos presentes, timpánico, blando y deprimible, doloroso a la palpación en fosa iliaca derecha, izquierda, región umbilical y epigástrica.
In the upright abdominal X-ray, only the distended abdominal loops are evident.
As a separate explanation, it is noted that they were in movement, in such a movement that the loops are not arranged in their normal position but are shown below the liver and the left hypochondrium, the peristalsis of the intestinal loops that causes the movement is at such an increase that causes the colicky pain that the patient has.

Imagen realizada en illustrator cs6 de mi autoria.
Image made in illustrator cs6 of my authorship.
Se colocó un laxante de glicerina evidenciándose evacuaciones efectivas abundantes y alivio de la distención y el dolor.
Imagen realizada en illustrator cs6 de mi autoria.
Image made in illustrator cs6 of my authorship.
El paciente se dio de alta con antiespasmódicos y cambios de estilo de vida, indicándole la importancia de la ingesta abundante de agua, el ejercicio físico y una dieta saludable con disminución de las grasas y la sal y aumento de las fibras de tipo vegetales y verduras, avena.
Este es un caso de estreñimiento en donde en algunas ocasiones este trastorno puede causar innumerables molestias llegando a producir cuadros severos, su manejo inicial se basa en cambios de estilo de vida y solo al no obtener mejoría el inicio de tratamiento farmacológico con laxantes.
La alimentación. El uso de fibra deriva sobre todo de, trigo, así como algunos cereales como la avena. El más conocido es el trigo integral, que puede ser ingerido como parte de la dieta habitual. La fibra dietética aumenta el bolo fecal y la frecuencia, y reduce el tránsito medio intestinal.
La ingesta de agua ayuda al estreñimiento y el ejercicio puede aumentar el tránsito colónico en voluntarios sanos, Los posibles mecanismos por los cuales actúa el ejercicio sobre la motilidad intestinal parecen estar relacionados con estimulación de la liberación de péptidos y hormonas, y con mejoría de la perfusión del tracto gastrointestinal.
Y este trío de dieta saludable con aumento de fibras, buena ingesta de agua y ausencia de sedentarismo es nuestro manejo inicial del paciente.
This is a case of constipation where on some occasions this disorder can cause innumerable discomforts, leading to severe symptoms. Its initial management is based on lifestyle changes and only when no improvement is obtained is the start of pharmacological treatment with laxatives.
Feeding. The use of fiber derives mainly from wheat, as well as some cereals such as oats. The best known is whole wheat, which can be eaten as part of the usual diet. Dietary fiber increases fecal bolus and frequency, and reduces mid-intestinal transit.
Water intake helps constipation and exercise can increase colonic transit in healthy volunteers. The possible mechanisms by which exercise acts on intestinal motility seem to be related to the stimulation of the release of peptides and hormones, and with improvement of the perfusion of the gastrointestinal tract.
And this trio of healthy diet with increased fiber, good water intake and absence of a sedentary lifestyle is our initial management of the patient.

Imagen realizada en illustrator cs6 de mi autoria.
Image made in illustrator cs6 of my authorship.

Imagen realizada en illustrator cs6 de mi autoria.
Image made in illustrator cs6 of my authorship.
Si me quieren apoyar también en mi instagram y les gusta mi contenido y quieren que trabaje más en la medicina ilustrada aquí les dejo
Cacture de pantalla de mi instagram médico. @dramariagp en instagram
Screenshot of my medical instagram. @dramariagp by instagram.